Most supplement stacks do not fail because the person running them lacks discipline. They fail because the protocol was designed for someone else's biology, someone else's schedule, and someone else's goals — and then measured against a feeling instead of a number.
These ten principles cut through the noise with what the research actually supports, and more importantly, what your own data can confirm.
- 01Method beats ingredient list. What separates stacks that work from stacks that do not is the loop around them — baseline, intervention, measurement, review — not the specific compounds inside.
- 02Personalize from a 14-day baseline, not a template. Two weeks of stable logging before any change is your personal control group and the only thing that makes individual response legible.
- 03Rank by evidence strength before you buy. Start with Tier 1 compounds that have multiple RCTs or position stands behind them. Move down the evidence ladder only after the top is exhausted for your goal.
- 04Timing is a free variable with large effects. Matching each compound to its circadian window — stimulants early, GABAergics late, fat-soluble vitamins with meals — changes outcomes without changing dose.
- 05Cycle anything that downregulates itself. Stimulants, adaptogens, and receptor agonists need scheduled off-cycles and washouts to keep the response measurable over time.
- 06Check medications and interactions first, always. Interaction risk and duplicate ingredients kill more stacks than under-dosing. Run the screen before the first dose, not after a side effect.
- 07Adherence is the real constraint. A simple stack you hit 95% of the time beats a clever stack you follow 60% of the time. Complexity has to earn its place on measurable outcomes.
- 08Log every dose on-device, in the moment. Memory overestimates intake by 20–40% at the end of the week. HealthKit-backed one-tap logging is the difference between a protocol and a guess.
- 09Run each stack as an n-of-1 experiment. Baseline, ramp, run, review, stop rule. Treat every change as a single-variable test with a pre-declared decision.
- 10Review on a cadence or your stack drifts. Weekly stack review and quarterly deload catch compounds that stopped serving you before they become permanent residents.
The Truth About Supplement Stacks Right Now
Decades of supplement research converge on a frustrating conclusion. No single stack works for everyone, and the compounds with the strongest population-level evidence still have wide individual response windows. What reliably separates people who get results from people who do not is not the ingredient list. It is the method.
Personalization from baseline data, evidence-graded prioritization, honest dose timing, planned cycling, adherence-first design, medication safety checks, structured n-of-1 experimentation, foundational nutrient sufficiency, on-device logging, and scheduled review keep appearing across clinical literature, sports nutrition position stands, and real user data as the practices that move outcomes most.
This is not a 30-day protocol. It is the operating loop that Unfair was designed around — stacks as experiments, not shopping lists.
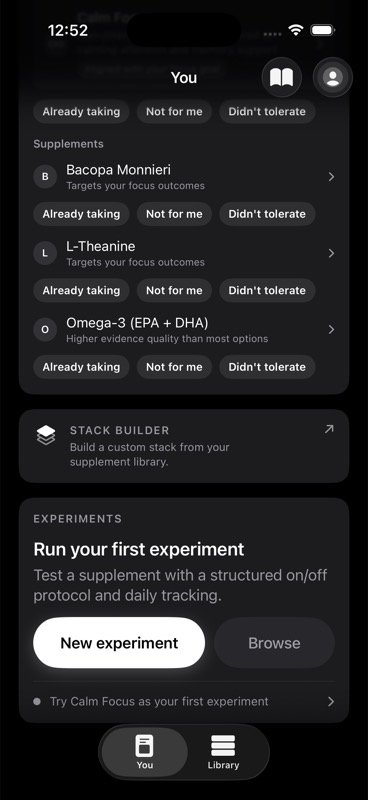
Start with what you already take. Build from there.
1. Personalize From Your Baseline, Not a Template
Log 14 days of outcomes and confounders before you add anything new.
A 2015 Weizmann Institute study in Cell tracked 800 people eating identical meals and found wildly variable metabolic responses from person to person.1 Supplement response has the same signature. Two people taking 400 mg of magnesium glycinate at 9pm can see completely different shifts in sleep onset because their baseline magnesium status, stress load, and sleep hygiene are different. A generic protocol cannot see any of that. Your own 14-day baseline can.
A desk worker on four hours of screen time after dinner and a shift-working parent eating at midnight will respond differently to the same bedtime dose window, even if the compound and dose are identical. The only way to know which effects are yours and which are noise is to measure yourself before you intervene.
2. Dose With Your Circadian Clock, Not Against It
Place each supplement in the window where its mechanism actually operates.
A 2019 Obesity trial on early time-restricted eating found that identical intake produced measurably different metabolic outcomes based on when it was consumed, because circadian rhythms govern hormone release, absorption, and receptor sensitivity on a 24-hour clock.2 Caffeine taken at 4pm does not behave like caffeine taken at 7am even at identical dose. Magnesium threonate at noon does not behave like magnesium glycinate at bedtime. Vitamin D taken with a low-fat breakfast absorbs differently than the same dose taken with a fat-containing meal.
The person who dumps their entire stack into a single morning capsule ritual is treating dose as a checklist instead of a schedule. Cortisol-supporting adaptogens want the morning, GABAergic compounds want the evening, and stimulants want a hard cutoff eight to ten hours before your target bedtime. Our Complete Guide to Dose Windows and Cycles covers the full schedule; the point here is that timing is a free variable with large effects.
3. Evidence-Grade Before You Buy
Rank candidates by strength of human evidence, not novelty or marketing.
The supplement market rewards novelty. Your biology does not. A 2017 International Society of Sports Nutrition position stand on creatine documents multi-decade RCT evidence for strength and high-intensity performance at defined doses.3 A 2021 ISSN position stand on caffeine does the same for alertness and endurance.4 These compounds are not interesting. They are the most reliably effective entries in the entire category. Ninety percent of "new" compounds do not have comparable evidence and will not for years.
Unfair's evidence graph — 271 supplements, 781 outcomes, 3,919 evidence edges — ranks candidates for your goal by actual evidence quality, not marketing cycle. The principle is simple: do not move down the evidence ladder until the top of it is exhausted or ruled out for you personally. A Tier 3 compound may work. It just has not been tested well enough to make it a rational first bet.
4. Cycle Intentionally To Preserve Response
Build off-cycles into any compound that downregulates its own target.
Tolerance is not a fringe concept. Caffeine tolerance develops within days to weeks and blunts the stimulant effect most people are actually paying for.4 For compounds with limited long-term daily-use data, including many adaptogens and sleep aids, periodic reassessment keeps the stack tied to observed benefit instead of habit.
A planned stack cycle — on-cycle, off-cycle, washout, then optional re-test — restores responsiveness and produces a cleaner second signal when you reintroduce the compound. The self-experimenter who runs their stimulant protocol 365 days a year is paying for a diminishing return they cannot see because the baseline has drifted with them. The one who cycles can actually tell whether the compound is still doing work.
5. Check Interactions and Medications First
Run a contraindication and duplicate-ingredient pass before the first dose.
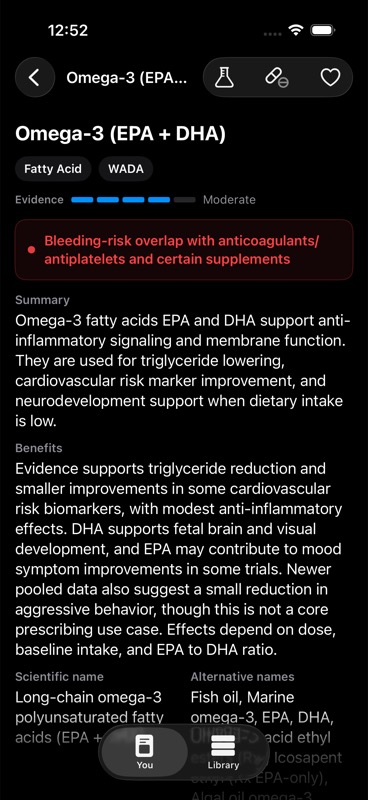
Supplement-drug interactions are not rare. St. John's wort induces CYP3A4 and can drop plasma levels of SSRIs, oral contraceptives, and immunosuppressants. High-dose omega-3 stacked with antiplatelet or anticoagulant medication shifts bleeding risk. Adaptogens with blood-pressure effects change the math on antihypertensives. Geller et al. estimated thousands of annual hospitalizations from dietary supplement adverse events, underscoring why interaction and contraindication checks need to happen before dosing.11
The Unfair recommendation engine screens for contraindication, interaction risk, and duplicate ingredient risk on every stack you build. Reviewing common supplement stack mistakes to avoid covers the concrete interaction checks to run. The pattern worth internalizing: medications first, then stack, never the other way around.
6. Protect Adherence Over Elegance
A simpler stack you actually take beats a clever stack you skip.
More frequent dosing and more complex regimens are consistently associated with poorer adherence in chronic therapy. Supplements are not medications, but the adherence curve is similar enough to matter. The consistency score Unfair tracks is the single best predictor of whether a stack will produce a signal you can act on.
The biohacker running an 11-compound, four-window-per-day protocol is not more serious than the one running a 4-compound, two-window protocol. They are running a harder experiment with more noise, lower adherence, and more confounders. Complexity has to earn its place. A minimum viable stack that you hit 95% of the time is the baseline every addition must beat on measurable outcomes.
7. Log Every Dose, On-Device
Capture dose events at the moment of dosing, not from memory at the end of the week.
Memory is a terrible data-capture mechanism. Recall studies on medication adherence consistently show that self-reported intake overestimates actual intake by 20 to 40 percent, and the gap widens with stack complexity. Without a dose log, you cannot separate "the compound did not work" from "I took it three times this week instead of seven." The manual dose journal plus one-tap logging closes that gap without requiring a spreadsheet or a habit overhaul.
Unfair writes dose events to HealthKit on-device. Nothing leaves the phone. That matters for two reasons: the privacy model makes the friction of logging acceptable long-term, and the HealthKit write produces a correlatable timestamp you can align against sleep, HRV, resting heart rate, and activity data from the same device. A one-tap dose logging action plus cycle-aware reminders produces a dataset that actually supports a decision at review time.
8. Build the Foundational Three Before the Exotic Stack
Confirm omega-3, vitamin D, and magnesium status before spending on anything novel.
The VITAL trial found overall neutral primary cardiovascular and cancer endpoints for omega-3 supplementation, with signals in subgroup analyses for people with low baseline fish intake.5 Vitamin D insufficiency affects roughly 40% of American adults and is associated with immune, metabolic, and mood endpoints across large cohorts.6 Magnesium is involved in hundreds of enzymatic reactions and is systematically under-consumed in Western diets, with randomized evidence for sleep and blood-pressure endpoints in deficient populations.89
The person running a seven-compound nootropic protocol without knowing their vitamin D level is optimizing blindly. A single standard panel costs less than a month of indiscriminate supplementation and tells you where your foundation supplement layer actually needs to sit. Exotic compounds layer on top of foundation sufficiency, not around it.
9. Run Each Stack as an N-of-1 Experiment
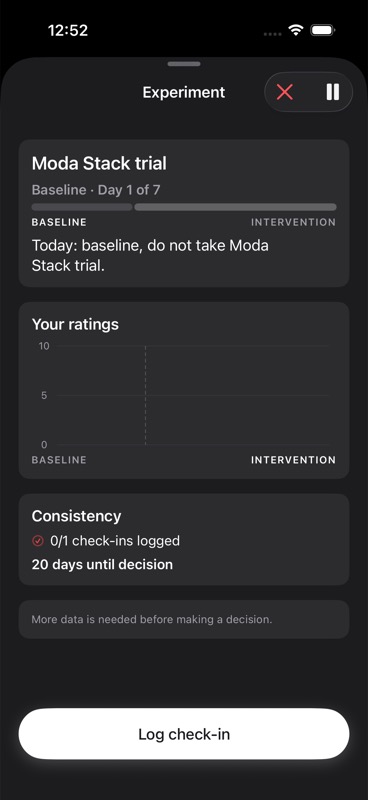
Commit to a baseline, ramp, run, and review window with pre-declared stop rules.
The CONSORT extension for N-of-1 trials, published in 2015, codifies what responsible single-person experimentation looks like: a stable baseline, a controlled intervention, a planned observation window, and a pre-declared decision rule.10 The tooling cost of doing this has historically been the blocker. People who self-experiment seriously end up maintaining a spreadsheet for exactly one quarter before it collapses. The ones who stay rigorous use software that enforces the structure for them.
Unfair's experiment flow pairs a stack with an outcome metric, a baseline window, a ramp, and a stop rule. The decision at the end is binary: the signal was large enough to keep the stack, or it was not. The parent who adds rhodiola and also starts sleeping 45 minutes more every night has confounded the experiment. The one who held sleep, training, and caffeine constant across the baseline and intervention window has an answer.
10. Review and Deload on a Cadence
Schedule a weekly stack review and a quarterly deload, and keep them on the calendar.
Stacks do not fail catastrophically. They drift. A compound that served you in a training block stops making sense in a recovery block. A sleep aid that worked through a stressful quarter becomes unnecessary. A foundational layer you added in the winter may be redundant in the summer when sun exposure is higher. Without a weekly stack review and a quarterly deload, a stack accumulates the way a closet accumulates — by default, not by design.
The professional who has taken the same 9 compounds for 14 months without review is not disciplined. They are running a protocol that stopped being responsive to their life. Reviewing on a cadence — kept short, kept on the calendar, kept tied to logged data — is the difference between a stack that performs and a stack that merely persists. Our Complete Guide to Supplement Stacks walks through the full review rubric.
Where to Start
Do not try to apply all ten at once. That is how good ideas become abandoned plans.
Pick the two principles that map most directly to where your stack is weakest right now, and commit to them for three weeks. Log during the entire window. Review at the end.
If you do not know where to begin, start with principle 7 and principle 9 — log every dose on-device, and attach the next change you make to a single n-of-1 experiment with a defined window. Those two moves produce more signal in a month than a rewritten stack produces in a year.
The goal is not a perfect stack. The goal is a stack that stays honest — measured against your own data, revised on a cadence, and designed around the biology of the person actually running it.
References
Zeevi D, Korem T, Zmora N, et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell. 2015;163(5):1079-1094. https://pubmed.ncbi.nlm.nih.gov/26590418/
↩Sutton EF, Beyl R, Early KS, et al. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss. Cell Metab. 2018;27(6):1212-1221. https://pubmed.ncbi.nlm.nih.gov/29754952/
↩Kreider RB, Kalman DS, Antonio J, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation. J Int Soc Sports Nutr. 2017;14:18. https://pubmed.ncbi.nlm.nih.gov/28615996/
↩Guest NS, VanDusseldorp TA, Nelson MT, et al. International Society of Sports Nutrition position stand: caffeine and exercise performance. J Int Soc Sports Nutr. 2021;18:1. https://pubmed.ncbi.nlm.nih.gov/33388079/
↩Manson JE, Cook NR, Lee IM, et al. Marine n−3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N Engl J Med. 2019;380:23-32. https://pubmed.ncbi.nlm.nih.gov/30415637/
↩NIH Office of Dietary Supplements. Vitamin D: Fact Sheet for Health Professionals. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
↩NIH Office of Dietary Supplements. Magnesium: Fact Sheet for Health Professionals. https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/
↩Abbasi B, Kimiagar M, Sadeghniiat K, et al. The effect of magnesium supplementation on primary insomnia in elderly. J Res Med Sci. 2012;17(12):1161-1169. https://pubmed.ncbi.nlm.nih.gov/23853635/
↩Vohra S, Shamseer L, Sampson M, et al. CONSORT extension for reporting N-of-1 trials (CENT) 2015 Statement. BMJ. 2015;350:h1738. https://www.bmj.com/content/350/bmj.h1738
↩Geller AI, Shehab N, Weidle NJ, et al. Emergency Department Visits for Adverse Events Related to Dietary Supplements. N Engl J Med. 2015;373:1531-1540. https://pubmed.ncbi.nlm.nih.gov/26465986/
↩